James Maitland is a distinguished authority in the integration of robotics and Internet of Things (IoT) applications within modern medicine. With a career dedicated to advancing cardiovascular solutions through high-tech interventions, he has closely monitored the evolution of mechanical circulatory support. His insights provide a critical perspective on the recent clinical shifts surrounding heart pump technologies and the necessity of data-driven patient selection in high-stakes cardiac procedures.
In complex percutaneous coronary interventions, data indicates higher mortality rates and no reduction in adverse events when using mechanical support compared to standard procedures. How do you interpret these mortality signals, and what specific clinical indicators should now determine which patients actually warrant this technology?
The mortality signals observed in the CHIP-BCIS3 trial are deeply sobering, particularly the finding that 47 patients in the pump group passed away compared to only 33 in the PCI-only group. When you see that patients without a pump fared better in 43% of comparisons, it suggests that the added complexity and physical presence of the device may introduce risks that outweigh its hemodynamic benefits. We have to move away from the assumption that a reduced workload for the heart automatically translates to better survival in every complex case. Instead of routine use, clinical indicators should focus on patients where the procedural risk is truly insurmountable without support, rather than applying it broadly to all cases of severe left ventricular dysfunction.
When treating heart attack patients who are not in cardiogenic shock, resting the heart with a pump before stenting has failed to reduce muscle damage while increasing bleeding risks. How should medical teams weigh these trade-offs, and what specific safety protocols must be prioritized during these procedures?
The STEMI-DTU trial highlights a frustrating reality where the 30.8% rate of device-related major bleeding or vascular complications exceeded the performance goal of 26.5%. When you consider that muscle damage was essentially identical—30.8% with the pump versus 31.9% without—the trade-off clearly leans toward unnecessary harm for the patient. Medical teams must prioritize rigorous access-site management and real-time monitoring of vascular integrity to mitigate these bleeding risks. Moving forward, the protocol should mandate that mechanical support is reserved for those in cardiogenic shock, where the device is life-saving, rather than using it as a preemptive “rest” tool for stable heart attack patients.
Mechanical circulatory support is a massive growth driver in cardiovascular care, yet evidence now suggests a more selective approach is necessary for high-risk interventions. How can hospital systems transition away from routine use, and what step-by-step criteria should they implement to ensure evidence-based patient selection?
Hospital systems are in a difficult position because these devices contributed $1.75 billion to sales in 2025, signaling how deeply they are embedded in current cardiovascular business models. To transition away from routine use, systems must implement a multidisciplinary “Heart Team” review for every non-emergency high-risk PCI to ensure the device is truly necessary. The criteria should involve a step-by-step assessment of coronary anatomy, the degree of left ventricular dysfunction, and a frank discussion of the 36.6% success rate for pump-supported patients versus the higher success seen without them. We need to foster a culture of shared decision-making where the potential for harm, as noted by the trial investigators, is given as much weight as the desire for technical support.
Some suggest that supporting the left ventricle before restoring blood flow might create a window for adjunct pharmacotherapies to reduce reperfusion injury. What specific drug classes show the most promise for this application, and how would you design a trial to measure their effectiveness alongside mechanical support?
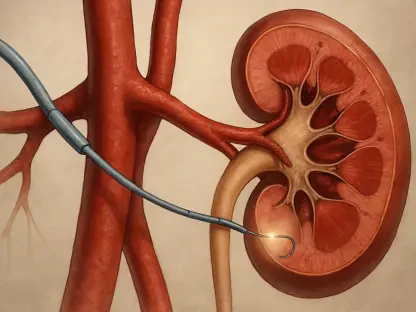
The idea that the Impella CP can maintain stability for over 40 minutes before blood flow is restored creates a unique “therapeutic window” that we haven’t fully exploited yet. I believe drug classes focused on mitochondrial protection or anti-inflammatory agents designed to blunt the sudden burst of oxygen radicals during reperfusion show the most promise. A trial to measure this would need to be a three-arm study comparing standard PCI, PCI with mechanical support alone, and PCI with mechanical support plus the adjunct therapy. By using the pump specifically to buy time for these medications to reach peak concentration before the stent is deployed, we might finally see a meaningful reduction in infarct size that has eluded us so far.
What is your forecast for the use of mechanical circulatory support in patients without cardiogenic shock?
I anticipate a significant cooling period where the routine use of these pumps in non-shock patients will decline as hospital protocols catch up to the CHIP-BCIS3 and STEMI-DTU data. We are likely to see a shift from “default support” to “rescue support,” where the device is kept on standby in the catheterization lab rather than being inserted at the start of every complex procedure. While the technology remains a vital tool for the sickest patients, its future in elective or stable cases will depend entirely on whether new trials can prove that the 40-minute window of ventricular unloading can be successfully paired with other therapies. If we cannot prove that this extra time leads to better muscle preservation, the industry will have to accept that, for many, less technology actually leads to better outcomes.